

Thuỷ tinh thể XL Optic Aspira-aXA
ASPIRA-aXA
Pseudophakic reliability for you and your patients
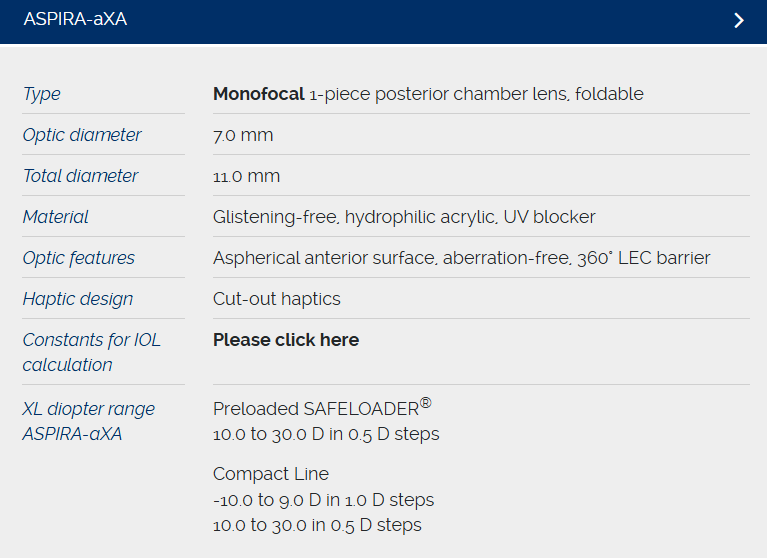
The innovative XL optic of the ASPIRA-aXA combines the advantages of a 7.0 mm optic with the stability of the new cut-out haptic design. This posterior-chamber IOL an be conveniently implanted using small-incision technology while adhering to surgical routine.
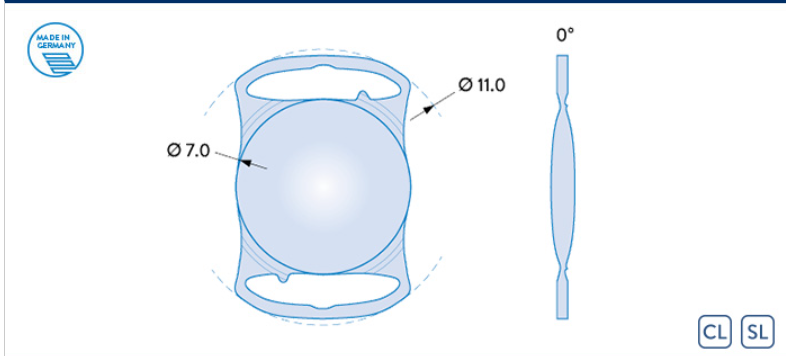
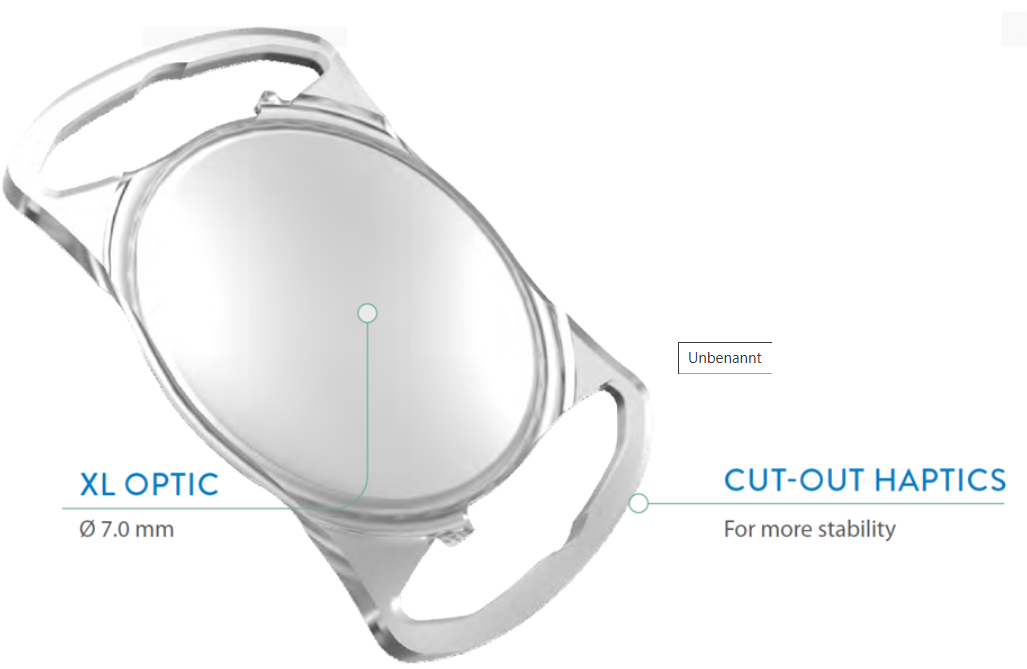
XL optic (Ø 7.0 mm) – XL reliability
XS incision – astigmatism-neutral through small incisions
XL easy preloaded SAFELOADER® – XS stress
ASPIRA-aXA
THE EXTENDED 7.0 mm XL-OPTIC
For standard cataract surgery and especially for patients with large pupils, traumatic mydriasis or iris defects
For patients at increased risk of retinal diseases or need for combined vitreoretinal surgery
EASY TO INTEGRATE INTO THE ROUTINE
Astigmatism-neutral implantation conveniently through small incisions
Precise and reliable IOL supply by preloaded SAFELOADER® autoloading system
Intuitive, easy handling for a quick and efficient surgical routine
FOR AN UNTROUBLED VISUAL OUTCOME
PREVENT PHOTIC PHENOMENA
Pseudophakic dysphotopsia is the most important dissatisfier for patients after successful cataract surgery.

BENEFIT FROM A SMOOTH ADAPTION PHASE
Reduced dysphotopsia from the early postoperative course leads to a fast adaption to the patient’s visual habits and results in high patient satisfaction
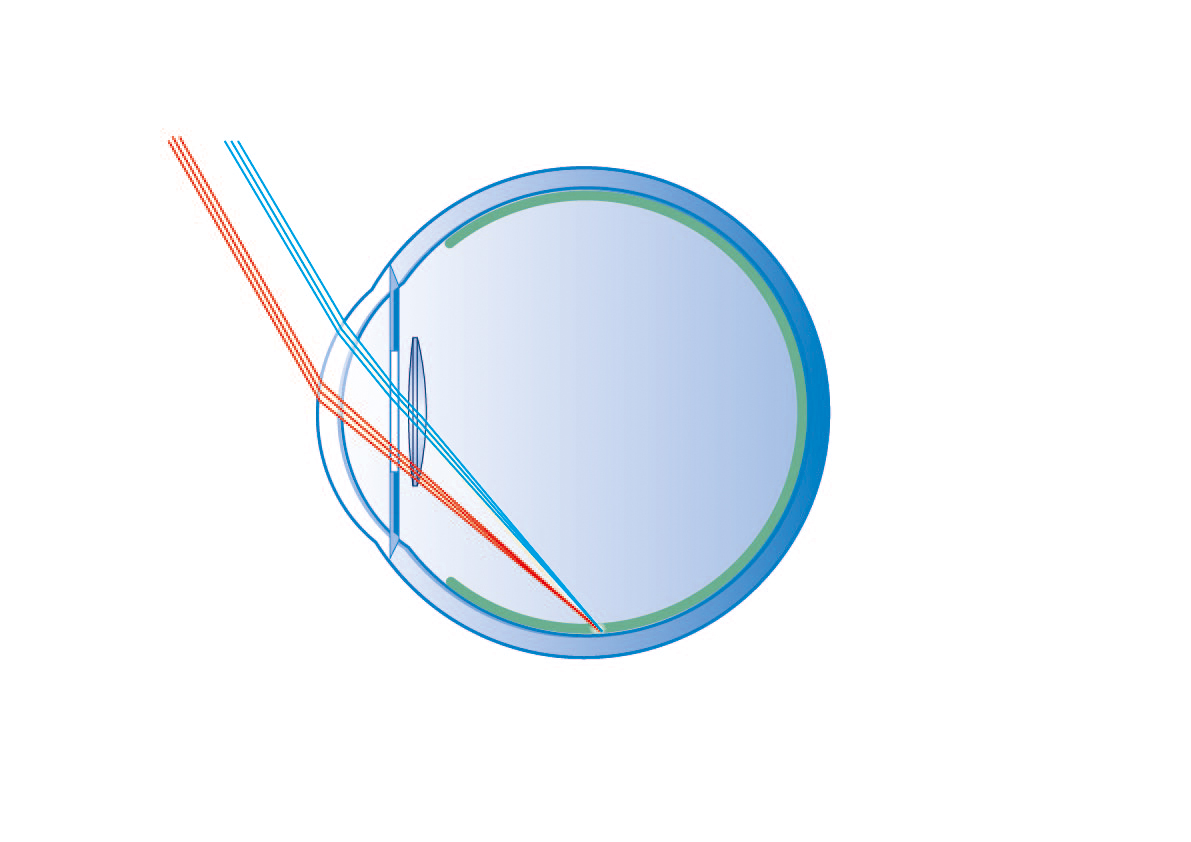
Overlap of pupil and IOL optic prevents light passing by the IOL. Incident light is safely directed through the XL-optic
Interfering edge effects get diminished, frequency and extent of dysphotopsia are reduced in comparison to conventional 6.0 mm IOL designs
PREVENT PERSISTENT DYSPHOTOPSIA
Bag-to-bag IOL exchange with the 7.0 mm Aspira-aXA showed complete resolution of dysphotopsia in almost all patients. An IOL exchange with a wide optic diameter IOL seems a promising surgical treatment for dysphotopsia.
Simulated beam guidance with a 6.0 mm optic
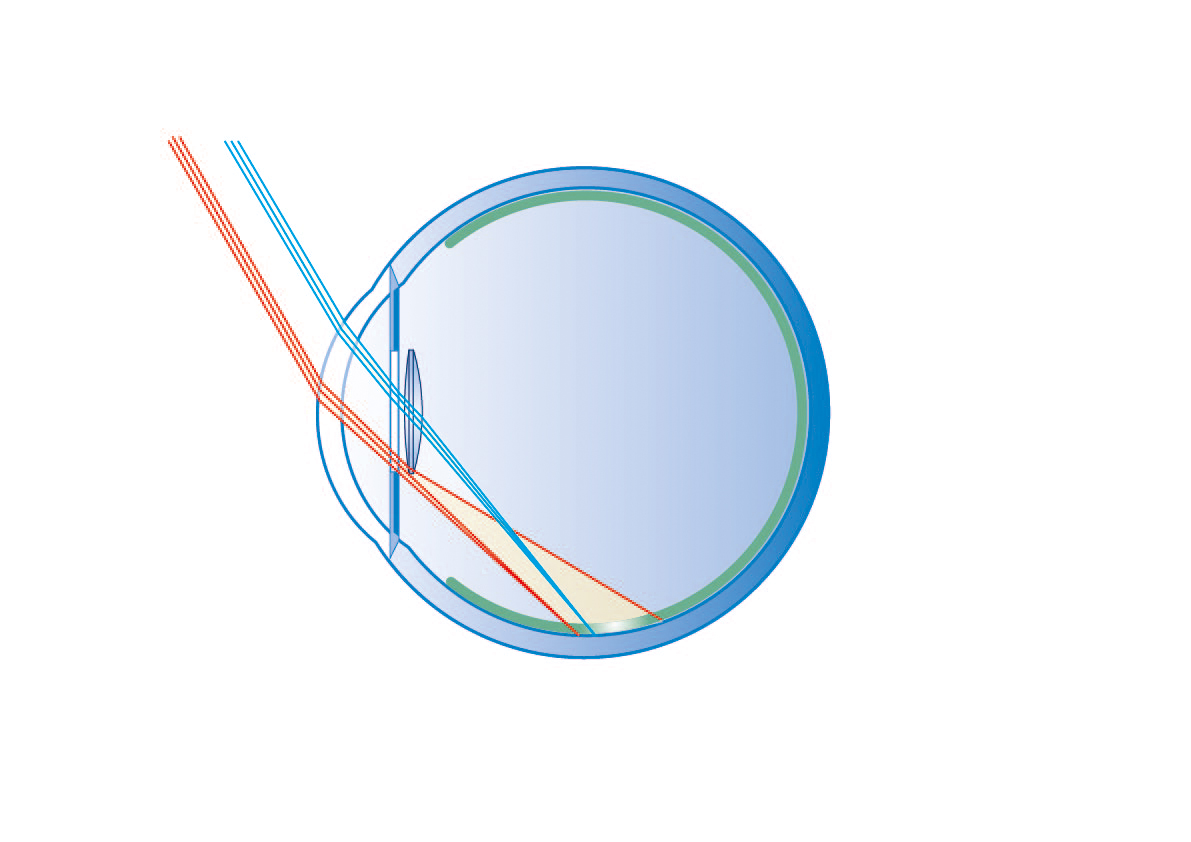
Simulated beam guidance with a 7.0 mm optic
A model
FOR THE DEVELOPMENT OF NEGATIVE DYSPHOTOPSIA
Numerous ray tracing analyses using standard IOLs show a non-illuminated region of the peripheral nasal retina. This “shadow” is caused by the reduced optic diameter and the central thickness of the artificial IOL compared to the natural lens.
Schematic drawing modified according to Holladay
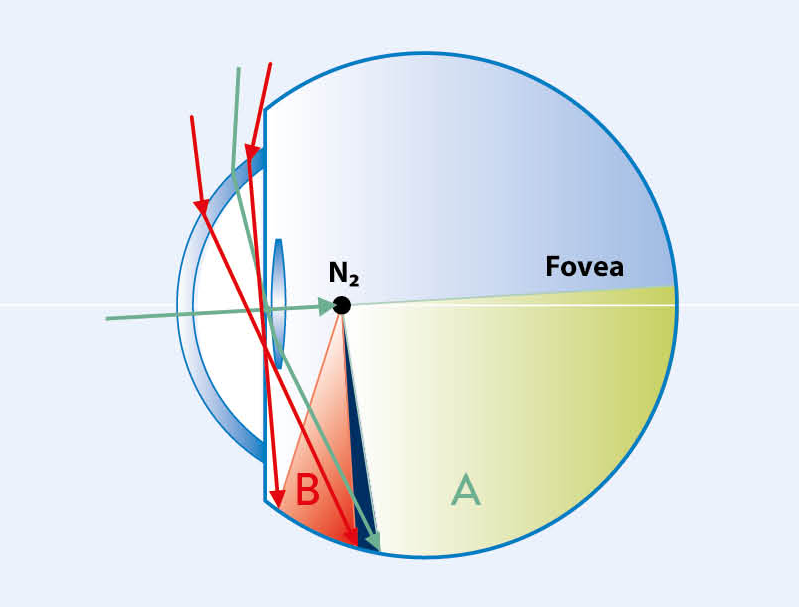
2.5 mm pupil, 6.0 mm IOL
The retinal image is generated by light rays refracted by the IOL optic (areal A), as well as by light rays that hit the retinal periphery (area B) either directly or indirectly refracted by the IOL edge. The unilluminated gap between these two areas can lead to the perception of negative dysphotopsia.
THE PANORAMIC IOL
THINKING ONE STEP AHEAD
THE SOLUTION FOR VITREORETINAL SURGERY
Possibility to perform wide capsulorhexis contributes to undisturbed wide view
XL diopter range from -10.0 D appointed to highly myopic patients
AN INVESTMENT IN THE FUTURE
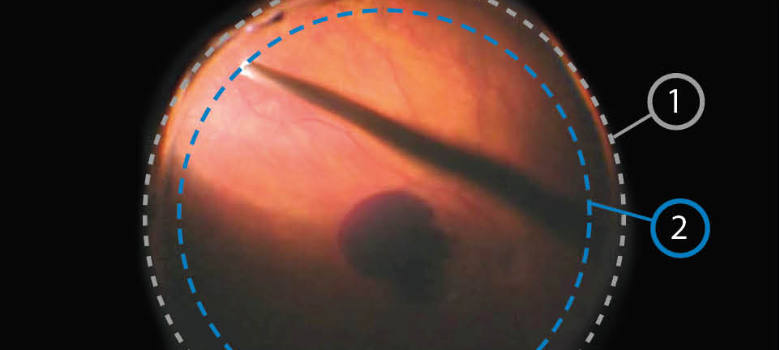
Intraoperative fundus image* (1) Edge of the XL optic (2) Theoretical optic edge of a 6.0 mm IOL
EXCELLENT INTRAOPERATIVE VIEW
Opening of the anterior capsule membrane with a rhexis diameter of up to 6.5 mm
Extended fundus view for convenient assessment of the tissue structures of the posterior segment of the eye
Facilitates therapeutic measures in the presence of peripheral retinal diseases
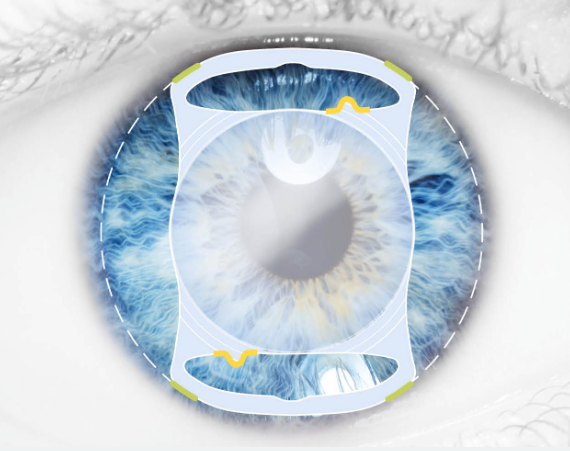
SAFE POSITIONING
STABLE REFRACTION
·
QUATTRO POINT CONTACT ZONE
Large contact area provides stability in the capsular bag
DOUBLE POSITION MARKING
For correct and safe placement
CUT-OUT HAPTICS
As absorption elements for embedding the IOL in the capsular bag
Dr. E. Becker, Oranienburg, Germany
“Aspira-aXA combines tilt-free fit, excellent A-constant fidelity with optical precision,
and its size makes it the number one monofocal IOL for eyes with a WTW greater than 12.0 mm and/or large pupils.”
Personal statement, 2023
Excellent overall capsular stability
Even in myopic eyes
Withstands increased pressure conditions providing stability also under extreme situations such as intravitreal injections or combined vitrectomies
CLINICALLY CONVINCING
Effective Reduction of Dysphotopsia
Incidence, frequency and extent of dysphotopsia are lower for patients treated with Aspira-aXA compared to patients treated with a 6.0 mm optic
Excellent Stability
Confirmed long-term stability with no significant IOL displacement or shift, hence no change in refraction
Highest Level of Patient Satisfaction
97 % of patients were highly satisfied or satisfied with their vision 1.5 years after surgery

Thuỷ tinh thể XL Optic Aspira-aXA
Còn hàng
Liên hệ
Thông số sản phẩm
Chính sách đổi trả
Hướng dẫn bảo quản
-

MIỄN PHÍ GIAO HÀNG TOÀN QUỐC
(Sản phẩm trên 300,000đ) -

ĐỔI TRẢ DỄ DÀNG
(Đổi trả 90 ngày cho Giày và 30 ngày cho Túi) -

TỔNG ĐÀI BÁN HÀNG 1800 1162
(Miễn phí từ 8h30 - 21:30 mỗi ngày)

TRIVAT Trifocal-toric IOLs
Liên hệ

Triva aA/aAY
Liên hệ

Aspira aA
Liên hệ


Thuỷ tinh thể Toric
Liên hệ

Aspira AAY
Liên hệ
TRIVAT Trifocal-toric IOLs
Liên hệ

The ARTIFICIALIRIS
Liên hệ

Chỉ polypropylene
Liên hệ
Chỉ Polyester
Liên hệ

Chỉ Silk
Liên hệ

Chỉ tiêu PGA
Liên hệ

Chỉ Nylon sợi đơn đen
Liên hệ


Thuỷ tinh thể XL Optic Aspira-aXA
Liên hệ
Kho:5000

Về đầu trang
